

I have been pondering the economics of an “anti-biofilm” agent. I received Plurogel samples from Medline and had dramatic success in a very compromised patient, both for her acute wound (due to an ulcerated hematoma) and her chronic ankle ulceration related to her thrombophilia. I’m struggling with the economic model, however.
We’ve analyzed thousands of wounds and have convincing data that systemic antibiotics help chronic ulcers heal. That’s a very inconvienent truth given the growth of antibiotic resistent bacteria. In truth, I am not at all convinced the same result could have been achieved in this patient with systemi antibiotics because the most impressive impact of the anti-biofilm agent was the resolution of significant undermining. However, if we pretend that the same effect could have been achieved with systemic antibotics, at least antibiotics are covered by most patients’ pharmaceutical benefit plan. One argument for using an antibiofilm agent is that less expensive dressings can be used, but most patients’ dressings are covered by their insurance. (Yes, there’s a lot of fine print around dressings nowadays– some Medicare Advantage plans are not covering dressings and the “Targeted Probes” have resulted in a lot of patients being sent hefty bills after the fact.)
You can argue that there is significant cost savings with an anti-biofilm agent in a “universal” sense if the time in service is reduced, but the patient has to pay cash for these agents and they can be hundreds of dollars per tube. This big out of pocket expense doesn’t “count” towards their insurance deductible. A lot of patients simply can’t afford to buy a product for hundreds of dollars, and the margin in a wound center or doctor’s office is too small to provide it FOR the patient.
If products like Plurogel really shorten time in service, then they could be hugely beneficial as CMS implements bundled payment models. However, paying hundreds of dollars cash out of pocket is a hard sell currently, even though the results of this case are impressive. It’s a sad reality that as it now stands, there’s reimbursement for a lot of very expensive things that are maginally effective in the real world, and no reimbursement for some (relatively low cost) products that make a big difference.
In a “bundled payment” world in which you got a fixed payment amount for a course of wound care, what would you include/provide that isn’t currently covered by insurance? Would you include an antibiofilm agent like Plurogel? Would your patients pay $200 a tube for a product like this?
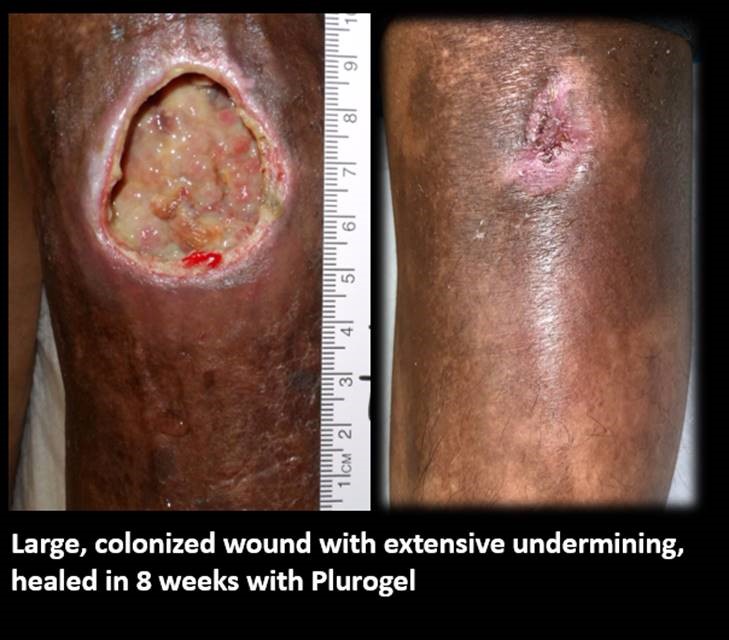
Here is the whole slideshow of Plurogel in a patient with Thrombophilia:

Dr. Fife is a world renowned wound care physician dedicated to improving patient outcomes through quality driven care. Please visit my blog at CarolineFifeMD.com and my Youtube channel at https://www.youtube.com/c/carolinefifemd/videos
The opinions, comments, and content expressed or implied in my statements are solely my own and do not necessarily reflect the position or views of Intellicure or any of the boards on which I serve.
