

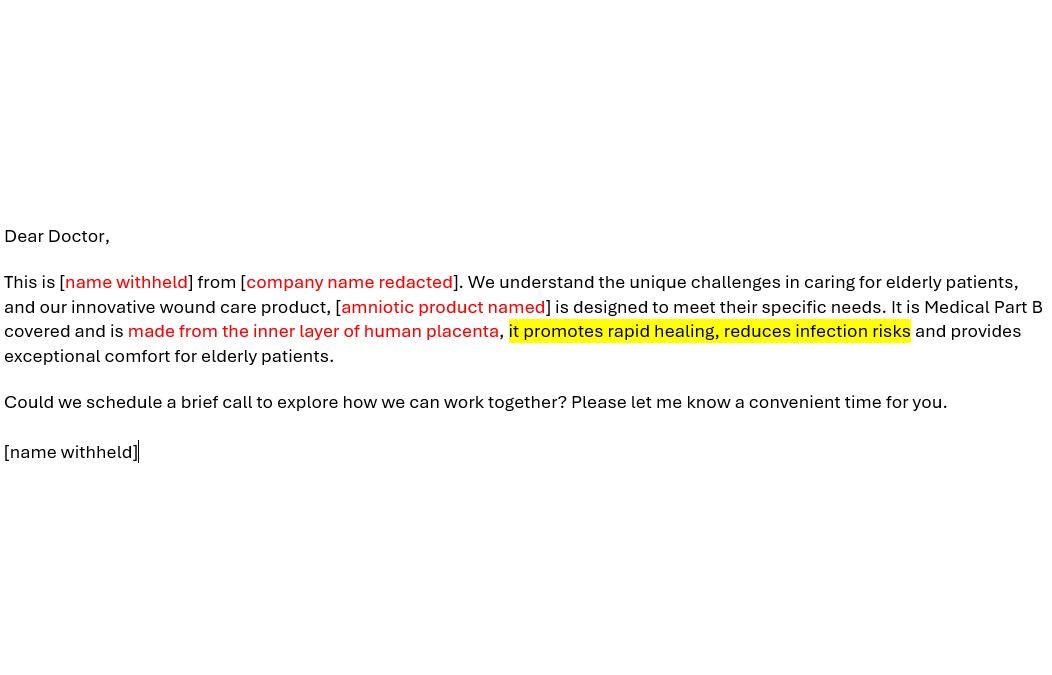
A few weeks ago, I got a message from a Cellular Tissue Products / skin substitute sales rep telling me about the great results seen using his product in Wagner grade 3 DFUs, specifically over bone and tendon. I wondered how he could make those claims given that, as far as I know, none of the CTP/skin subs have had a prospective trial of Wagner 3 DFUs. And then a colleague sent me a copy of the email above, referring to an amniotic product stating that it promotes rapid healing and reduces infection.
That got me wondering what specific claims that sales reps were allowed to make about CTPs/skin subs. I know that the short list of products which will be covered based on the proposed LCDs could change, but I thought it would be interesting to ask this question about the 15 products on the list. I decided to ask Joe Rolley about it, and here is his detailed answer.
Joe,
Using the list of the 15 skin substitute grafts/CTPs covered by Medicare in the proposed LCD(s), can you help me understand the different ways these products come to market, and how their path to market affects the claims about healing that a rep can make about them?
Caroline
Dr. Fife,
Before discussing paths to market, we first need to clarify nomenclature. There is a great deal of confusion about the terms that describe “skin substitutes” primarily because there are so many diverse types, so I will attempt to clear some of it up.
Let’s start with some basic terms:
- CTPs: Acronym that stands for Cellular and/or Tissue based Products for skin wounds. This is an all-inclusive term that refers to the entire category of skin substitute products regardless of source components and is the term currently accepted by ASTEM. This term has wide adoption and is preferred over the term “skin substitute.” (Note: A JWC International Consensus Document issued in April 2023 recommended the term Cellular, Acellular and Matrix‑like products [CAMPs] which many people prefer to CTP since it is less likely to be confused with the next term on this list – HCT/P)
- HCT/Ps: Stands for Human Cells, Tissues, and Cellular and Tissue-based Products intended for implantation, transplantation, infusion, or transfer into a human recipient and regulated by FDA Center for Biologics Evaluation and Research (CBER). HCT/P refers to a subset of CTPs that are sourced from human tissues.
- PHS Act: Section 361 of the Public Health Service Act (42 U.S. Code § 264) authorizes the U.S. Secretary of Health and Human Services to take measures to prevent the entry and spread of communicable diseases from foreign countries into the United States and between states. HCT/Ps are not subject to FDA pre-market approval (PMA) or 510(k) clearance rather they are subject to PHS Act Section 361 and are not required to be licensed or approved by the FDA.
- 510(k) medical device: Refers to Section 510(k) of the Food, Drug and Cosmetic Act. Manufacturers of 510(k) devices are required to notify the FDA Center for Devices and Radiological Health (CDRH) if they intend to market a medical device that is equivalent to one that is already approved or cleared by the FDA. This is the premarket notification
- Premarket Approval (PMA): FDA process of scientific and regulatory review to evaluate the safety and effectiveness of Class III medical devices where FDA has determined general and special controls alone are insufficient to assure safety and effectiveness. Skin substitutes that went through the PMA process represent first-to-market entrants prior to the availability of other previously approved or cleared skin substitutes.
Many people misunderstand the differences between human tissue-based skin substitutes (HCT/Ps) and those that came to market via the PMA or 510(k) medical device processes. It’s clear that there is a lot of confusion even within the industry. The regulatory pathways for human tissue-based (HCT/Ps) and “medical device” skin substitutes are quite different, and that means the FDA claims approval process for tissue-based products and medical devices are also quite different.
In this article we are not going to discuss how the various Medicare Administrative Contractors (MACs) evaluated the published evidence to decide whether a product was put on the “covered” list for the Local Coverage Determinations (LCDs)! We are only going to discuss how these products came to market and what that might mean about the claims that can be made about them.
HCT/Ps included in the current LCD(s)
As everyone knows, the list of skin substitutes on the market is long and keeps growing. However, you asked me to focus on the list of 15 products that would be covered by Medicare if the proposed LCD(s) are implemented as currently written. Although I realize that the list may change before the final rule, the “covered” list currently includes 9 skin substitutes which contain amniotic, placental, and other human-sourced tissues and thus are all considered HCT/Ps. These are: Affinity®, AmnioBand®, DermAcell®, Epifix®, Epicord®, FlexHD®/Allopatch®, Grafix®, GraftJacket®, and Theraskin®. These products fall under the Public Health Service (PHS) section 361 regulations and are considered “361 HCT/Ps”.
Products that are 361HCT/Ps do not have to go through the Premarket Approval (PMA) process to be approved by the FDA because they are “minimally manipulated” tissues which are intended for “homologous use”. Manufacturers of 361 HCT/Ps are only required to list their manufacturing establishments with the Public Health Service which reviews donor eligibility, current good tissue practice, and other procedures to prevent the introduction, transmission, and spread of communicable diseases by HCT/Ps. 361-exempt human tissue products are assumed to be safe if they are sourced from a tissue bank approved by The American Association of Tissue Banks (AATB) which certifies donor eligibility, current good tissue practice, and other procedures to prevent the introduction, transmission, and spread of communicable diseases.
If the FDA designates a product to be a minimally manipulated 361 tissue, there is no premarket approval or clearance performed by FDA. In other words, 361 products are not regulated as medical devices, but rather as minimally manipulated human tissues with no FDA-approved or cleared claims and indications. While it is true that differences in the way that tissues are processed during manufacturing can impact performance, any therapeutic claims about these products are limited to the same role the harvested tissue originally provided in the body (that is considered “homologous use.”) The fact that these products are exempt from the formal FDA approval or clearance process does not make them less virtuous than other products.
The FDA has determined that the role of tissue derived from umbilical cords and placentas is primarily to cover, cushion, and protect the surrounding tissue/fetus. Thus, manufacturers must be careful making claims about wound healing and say nothing definitive about healing but instead perhaps describe how their products have been used by clinicians and on what types of wounds. If a company promotes a bigger role than just “covering or protecting,” the FDA can reclassify it and require that the manufacturer go through submission to the premarket approval or clearance process.
Bottom line: 361 HCT/P skin substitutes do not go through official FDA clearance or FDA approval. They can technically be promoted for use to “cover and protect” any type or severity of wound but manufacturers of these devices cannot make specific claims about wound healing.
510(k) Medical Device CTPs included in the current LCD(s)
The LCD(s) covered list currently includes 3 skin substitutes that are classified by the FDA as 510k cleared medical devices. The 3 FDA cleared medical devices on the list are: OASIS® Wound and Tri-layer, and PriMatrix®.
The 510(k) (pre-market notification) process provides the FDA with documented evidence that a medical device is substantially equivalent to a predicate device; that is, a product that has already been approved for marketing by the FDA. A 510(k) device must demonstrate substantial equivalence comparing the new product with the predicate device based on laboratory testing and preclinical data. This process requires the manufacturer to demonstrate that the product is “safe and effective,” but human testing is usually not needed for 510k submissions. Information on design controls process, intended use, indications for use, design inputs, and design verification are all inputs for a 510k submission.
Bottom line: Products that have come through the 510(k) pre-market notification process can only be marketed for the indications (in this case, the wound types) cleared by the FDA for their predicate product.
PMA Approved Medical Devices included in the LCDs
There are only 3 skin substitutes on the market today that have gone through the Premarket approval (PMA) process, and these are: Apligraf, Dermagraft, Integra Dermal Regeneration Template/Omnigraft Dermal Regeneration Matrix. The requirements for PMA (Pre-market Approval) medical devices are much higher than for 510(k) submissions. Not only must the manufacturer demonstrate that a new device is “safe and effective,” but unlike 510(k) devices, they must also undergo human clinical trials that are approved by the FDA. The PMA process is a high bar for a product to achieve so it is not surprising that device manufacturers request the 510(k) pathway for their new products whenever possible. Just by way of example, Apligraf is indicated, ” . . .for use with standard diabetic foot ulcer care to treat full-thickness neuropathic diabetic foot ulcers of ≥3 weeks duration and which have not adequately responded to conventional ulcer therapy and extend through the dermis but without tendon, muscle, capsule or bone exposure.” In other words, the PMA process creates specific limitations on the way that a product is marketed. Each new indication for a PMA product requires a new PMA application and clinical trial.
Bottom line: Products that have come through the PMA process can only be marketed for the types and severity of wounds that were included in their prospective clinical trials and approved by the FDA.
How does the FDA pathway impact the claims made by reps?
The statutory mission of the FDA under the Social Security Act (SSA) is to determine the ‘safety and efficacy’ of drugs, biologics, and medical devices. The statutory mission of the Centers for Medicare and Medicaid (CMS) under the SSA is to determine whether a drug, biologic, or medical device is ‘reasonable and necessary’ for coverage. One could argue that CMS should only be requiring evidence of clinical effectiveness and not safety since safety is the job of the FDA. However, it may be fair to say that when CMS thinks about the question of safety, it is thinking about safety among their beneficiaries, most of whom are either over 65 or disabled, and who may represent a uniquely vulnerable group. In any case, this article was not about Medicare coverage but how the 15 proposed “covered” products in the proposed LCD(s) got to market, and how that might impact the claims that a sales representative can make about their product.
Because of their different pathways to market, not all skin substitutes included in the proposed LCDs have been subject to the same levels of regulatory scrutiny. That means clinicians should be cautious of the product claims made by exuberant sales representatives of the fifteen skin substitutes in the proposed LCDs.
Joseph Rolley, Principal
JTR Business Consulting, LLC
JTR.BusinessConsulting@gmail.com
This article represents the views and opinions of JTR Business Consulting, LLC. Nothing contained therein should be construed as providing medical advice, dictating reimbursement policy, or substituting the judgment of a practitioner. It is always the Provider’s responsibility to determine and submit appropriate codes, charges, and modifiers for services rendered.

Dr. Fife is a world renowned wound care physician dedicated to improving patient outcomes through quality driven care. Please visit my blog at CarolineFifeMD.com and my Youtube channel at https://www.youtube.com/c/carolinefifemd/videos
The opinions, comments, and content expressed or implied in my statements are solely my own and do not necessarily reflect the position or views of Intellicure or any of the boards on which I serve.

This article deserves a re-post as the various methods of how a product came to market have become relevant in today’s policy conversation. Great information here!