


This is a 70-year-old man with a dehisced flap on the plantar surface of the left foot after a melanoma excision 6 weeks earlier. Based on the photos that he showed me from his phone, the cancer surgeon struggled to close the large defect on the bottom of his foot because the excision required for this potentially deadly cancer was very large and the plantar foot is not a forgiving area. A few days after surgery he developed severe foot edema and copious wound drainage, and the flap came loose. When I examined him I found a deep wound on the left plantar foot with slough and several sutures that had torn through the macerated skin. I asked the patient what the surgeon was planning to do. He said that since the operation, all surgical follow-up visits had been virtual due to COVID.
On initial visit he was screened for arterial disease and his skin perfusion pressure was normal so I knew the reason couldn’t be arterial insufficiency. I discovered he has a history of idiopathic peripheral neuropathy which is probably familial. I controlled his edema with a foot wrap, debrided the slough, initiated advanced dressings, recommended nutritional supplementation with Vitamin D3 and 2 packets of L-arginine per day, and prescribed an off-loading sandal. We also taught his wife how to change his dressings. The wound was dramatically different in one week.
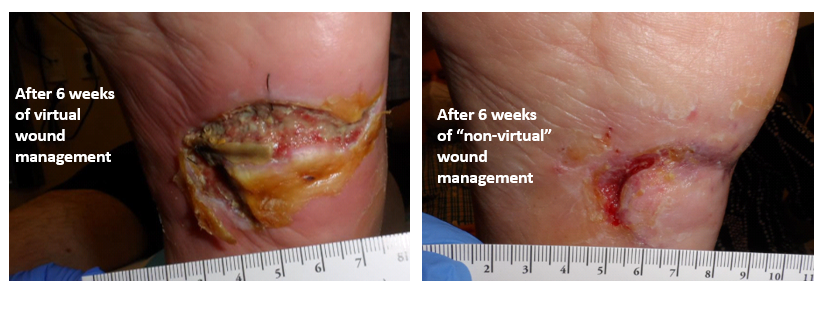
He was almost completely healed in 6 weeks. Would he have healed without my intervention? Probably – eventually. But I can understad why the patient and his wife were frightened by the appearance of the dehiscence and went looking for some “non-virtual” help for this wound.
I am all for flexibility in terms of how we do patient follow ups in the era of COVID, but it seems to me that virtual care has some limitations when it comes to wound management, particularly for a dehisced surgical wound. I’m afraid in this case, virtual post operative follow up was a disappointment. Our job is to find the reasons for a patient’s failure to heal and then correct them. Some of those interventions can’t be done virtually.

Dr. Fife is a world renowned wound care physician dedicated to improving patient outcomes through quality driven care. Please visit my blog at CarolineFifeMD.com and my Youtube channel at https://www.youtube.com/c/carolinefifemd/videos
The opinions, comments, and content expressed or implied in my statements are solely my own and do not necessarily reflect the position or views of Intellicure or any of the boards on which I serve.
