


A 44 year old woman presented with left arm and right lower leg ulcers that had been present for over 3 years. She has been seen by many specialists and treated with multiple courses of oral antibiotics, oral steroids, topical steroids, and advanced dressings. She was recommended to have venous ablation for her venous reflux. However, the lesions are not venous. The wounds on both her leg and her arm follow a dermatomal distribution (C7 and L5 nerve roots). She has constant itching of the skin in this area and she scratches herself, leaving open sores. She has known severe spinal arthritis which has probably caused nerve root compression and the resulting dysesthesia is perceived by her as itching. But, why can’t she heal these scratches?
She has hyper-flexibility of her joints and a positive wrist sign (see photo), crowded teeth and arachnodactyly of both hands and feet.


Her father died of a ruptured aortic aneurysm. What are these wounds a symptom of? Marfan’s Syndrome, one of the genetic collagen deposition disorders. The lesions are self-inflicted due to scratching the skin affected by the L5 nerve root compression, and due to her inability to make normal collagen, she can’t heal the areas of trauma as fast as she makes them. All I did was to cover her leg with an Unna’s boot to keep her from scratching, and in a few days, the wounds had closed by more than half. Here’s a photo before and after 7 days in an Unna’s boot.

I referred her to the medical genetics department since she has children with a similar phenotype and needs screening for an aortic aneurysm. She’d seen a lot of experts, but no one asked the question, “What are these a symptom OF?”
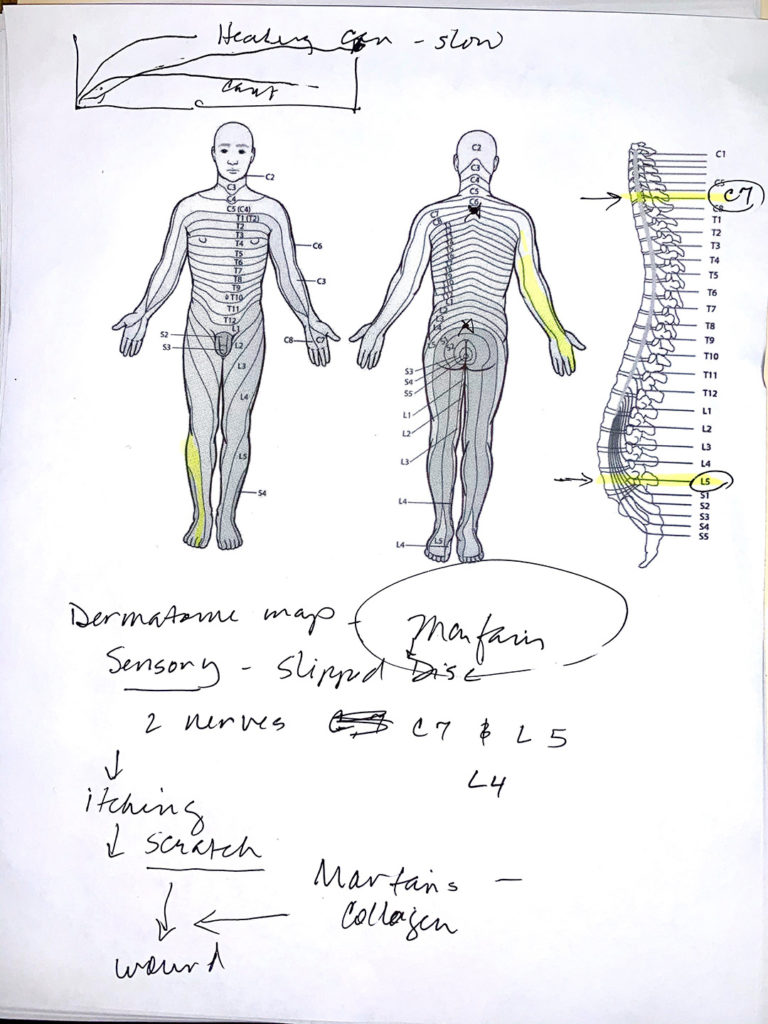
I do “sketch talks” with patients to make sure they understand the underlying disease process that causes their wounds – so we can agree on how and why to implement a specific treatment. Here’s my “sketch talk” for her.

Dr. Fife is a world renowned wound care physician dedicated to improving patient outcomes through quality driven care. Please visit my blog at CarolineFifeMD.com and my Youtube channel at https://www.youtube.com/c/carolinefifemd/videos
The opinions, comments, and content expressed or implied in my statements are solely my own and do not necessarily reflect the position or views of Intellicure or any of the boards on which I serve.

Very interesting! I was wondering if you also considered Ehlers-Danlos? Was it genetic testing that revealed Marfan’s diagnosis or did you rule out things & diagnose based on symptoms?
Can Mrafans syndrome lead to venous insufficiency?