


This is a 37 yo man with a non-healing wound at the site of a left chest catheter port. He has non-Hodgkin’s lymphoma and the port for his chemotherapy was removed 4 weeks after it was put in because it looked infected. He has had an extensive region of erythema and pain over the chest for more than 3 months that did not improve with several weeks of IV Vancomycin. Interestingly, the erythema gets better every time he received steroids in conjunction with his chemotherapy. Cultures (including a DNA assay for unusual pathogens) were negative and he has minimal drainage.
There is an extensive area of undermining and a lot of fat necrosis of the chest wall. A biopsy revealed fat necrosis without neutrophilic or histiocytic infiltrate- meaning, there’s no indication that the lesion is inflammatory (which was my first thought).

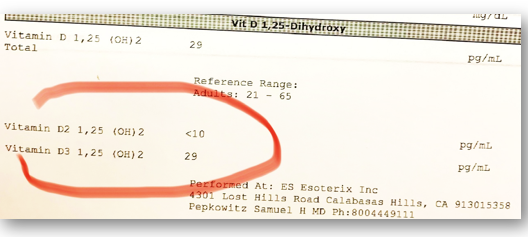
His Vitamin D-OH level is only 29 (30 is the minimum for healing) and he’s lost 55 lbs with chemotherapy, so we started Vitamin D3 supplementation and Juven.
It’s a lot easier to treat a wound when you know what it is. He might have been saved 6 weeks of IV antibiotics if there had been a bit more effort put into his diagnosis when cultures were negative and the antibiotics weren’t helping. This chronic ulcer was caused by extravasation of his chemotherapy agent into the tissues adjacent to the port. The best option for him, given the extensive fat necrosis on the chest wall, was a surgical excision and closure by a plastic surgeon (Dr. Kyle Gordley, who is superb at reconstruction procedures (Gordley Plastic Surgery), which went well, in part thanks to nutritional supplementation.


Dr. Fife is a world renowned wound care physician dedicated to improving patient outcomes through quality driven care. Please visit my blog at CarolineFifeMD.com and my Youtube channel at https://www.youtube.com/c/carolinefifemd/videos
The opinions, comments, and content expressed or implied in my statements are solely my own and do not necessarily reflect the position or views of Intellicure or any of the boards on which I serve.
