


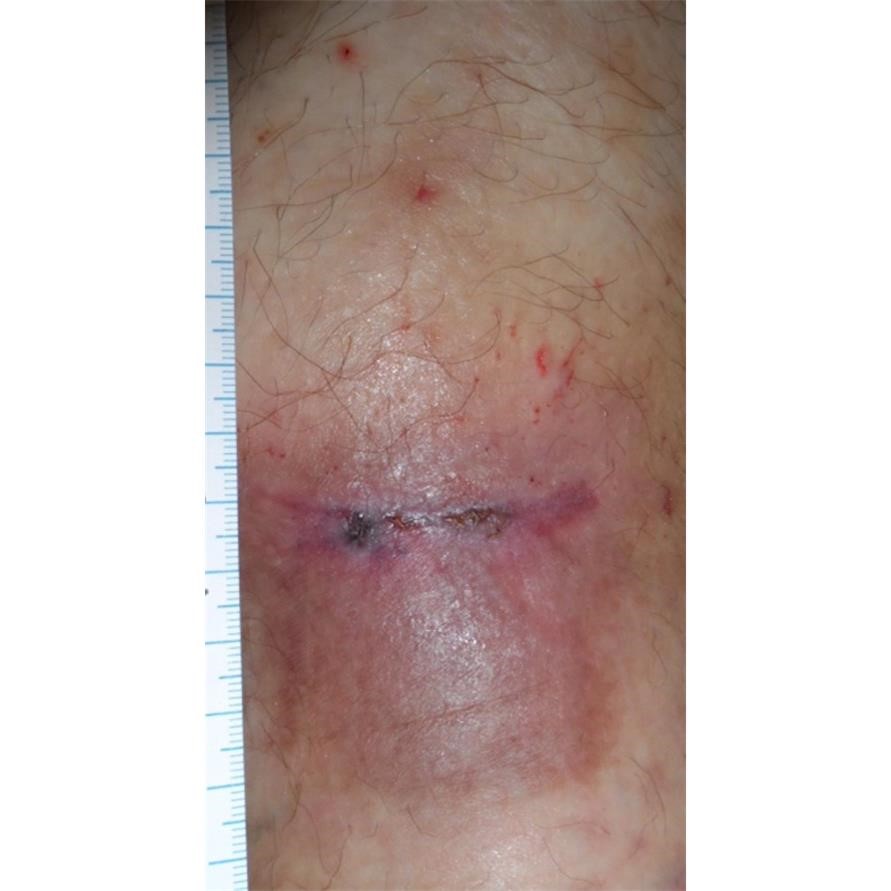
39 y.o. woman with a non-healing left anterior shin ulcer which had been present for a year after minor trauma. Her father and her daughter have autoimmune diseases but she has no such diagnosis, nor does she have joint pain or bowel problems. The wound began as a red dot which she scratched, after which it continued to enlarge until she could stick her pinky finger into the hole. It is painful and has not improved with any treatment over the past year including various antibiotics and topical preparations. She has no arterial disease or other underlying conditions except that she is overweight.
She was given a trial of Prednisone, and after one week had begun to have granulation tissue. She also underwent compression bandaging. Importantly, I DID NOT DEBRIDE THIS WOUND. DEBRIDEMENT MAKES PG WORSE. Use dressings for autolytic debridement. After confirming that her G-6-PD level was normal, she was transitioned from Prednisone to Dapsone and she healed about 8 months later.



The lesion returned after she stopped Dapsone but she returned quickly, Dapsone was restarted after a week of prednisone, and we agreed she would stay on a low dose of Dapsone after she healed for a year, with regular checks of her H&H since it can cause anemia.
My purpose is not to discuss the challenges of treating PG, but to show some of its many faces.

Dr. Fife is a world renowned wound care physician dedicated to improving patient outcomes through quality driven care. Please visit my blog at CarolineFifeMD.com and my Youtube channel at https://www.youtube.com/c/carolinefifemd/videos
The opinions, comments, and content expressed or implied in my statements are solely my own and do not necessarily reflect the position or views of Intellicure or any of the boards on which I serve.

I have had PG for 3 years now. I do not have an autoimmune disease, but I do have hEDS which contributes to slow healing. My shin was barely injured when I was working outside – the very top layer of skin peeled off like a sunburn. Within a week it was a dime-sized hole. It now measures 9cm x 7cm. My other leg has had PG for almost 2 years. Again the top layer of skin peeled off, but this time it was after surgery to repair a broken tibia. The surgical site healed PERFECTLY. Barely a scar! But I had intense edema and then it dissipated quickly, leaving loose skin. 12 small spots had the sunburn-type peeling of my skin. In a week I had 12 holes. They have all grown together, so I have one giant wound that is around 18cm x 12cm. Nothing is working to heal me. My wound care doc is beyond frustrated. I’ve even had 40 dives in the hyperbaric chamber.
This disease is so frustrating and PAINFUL. There is no reason my body should react like this, I don’t understand why I suddenly developed this. Those of us with this for years have many stories to share if someone would listen. We lose so much to it, because we have to quit our jobs, our hobbies, social lives, we lose our money, self esteem, and the desire to live.