


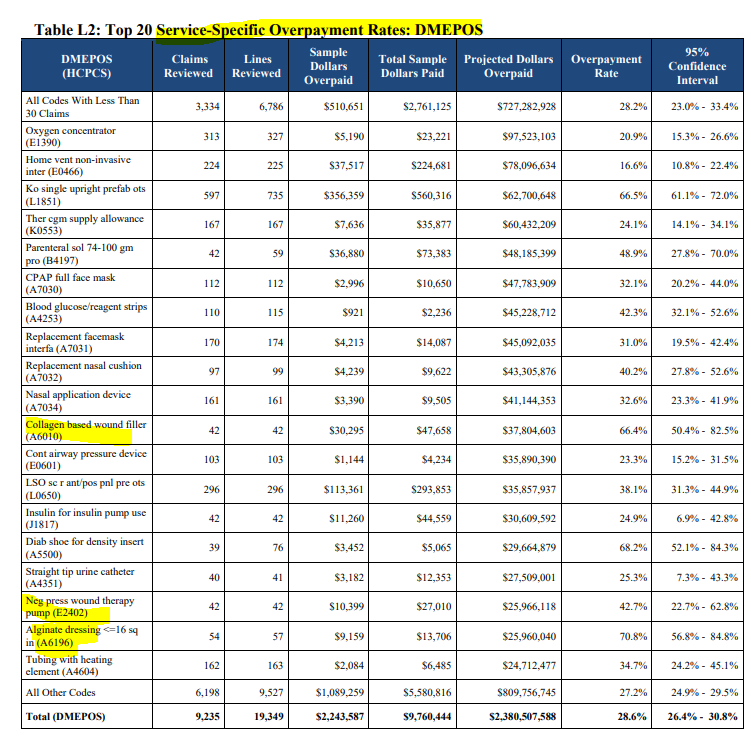
A few days ago, I got one of those CMS “eblasts” about the results of Medicare CERT audits (Comprehensive Error Rate Testing). The audit looks at whether there is sufficient documentation to back up the claim against Medicare. In 2021, CMS estimated that, based on data from the CERT audits, 6.26% of Medicare funding was incorrectly paid out — totaling $25.03 billion. The vast majority of those incorrect payments (64.1%) were marked as incorrect because the chart had insufficient documentation. I decided that I’d just skim the 2021 report and see if anything jumped out at me. I was surprised to see surgical dressings on the list.
Collagen dressings had an overpayment rate of 66.4% and alginate dressings of 70.8%. Here’s the scariest part, only 40 or 50 charts were reviewed to determine the overpayment rate on those two surgical dressings, but the results were extrapolated to indicate that over $37 million had been paid out improperly for collagen dressings and $25 million for alginate dressings. Remember that the doctors and clinics don’t end up being asked to pay back this money – the DMEs are on the hook for it. And remember that the audit doesn’t indicate that the patient’s didn’t NEED the dressings, only that there wasn’t enough documentation to support the claim. I just posted an editorial about this on Today’s Wound Clinic.
The bottom line is that DMEs are requiring very specific clinical documentation to support the orders they get, and when they can’t get the documentation, they don’t send dressings to the patient. Doctors and nurses are being driven crazy with documentation requests. I wanted clinicians to understand why this has become such a huge problem.
Here are a few examples of the charting problems:
- Mrs. Jones was seen today for her stage 3 pressure ulcer, which was almost 100% granulated. She had previously been treated with an antimicrobial dressing, but the care team decided that it was the perfect time to start a collagen, so this was ordered from the durable medical equipment (DME). However, at today’s visit, the patient requested that a foam with a film dressing be placed over the wound because she was going home to take a shower. Because the clinic note and the treatment plan did not specifically state that the plan was to use a collagen, and because a different category of dressing was documented as being placed today, if the DME provided a collagen, an audit it will be considered an improper payment.
- Mr. Smith has 2 large venous leg ulcers (VLUs) that drain copiously. He is being treated with an alginate covered by an absorbent secondary dressing. He had had to change his dressing just before coming to clinic because it was saturated, so at his visit, the clinical team documented his drainage as minimal. An alginate and absorbent secondary dressing were ordered from the DME, but because the nurse did not record the drainage as being moderate to large, if audited, these absorbent dressings will be considered improperly paid.
- Mr. Doe was seen for his very painful arterial ulceration. Due to pain and ischemia, sharp debridement of necrotic material is not an option. He has been tolerating enzymatic debridement and the amount of necrotic material is decreasing. The clinical note states that no debridement has been performed even though autolytic debridement has been used. If audited, the DME will have provided dressings improperly to this patient because the record does not state that the wound underwent autolytic debridement.
- Mrs. Doe has several large wounds and is dependent on the dressings supplied by the DME to care for her wounds at home. The clinical staff do an excellent job of care but are often behind at signing off the chart. The DME received the orders for all the supplies and called the clinic to request that the most recent notes be faxed to them. The final documents cannot be generated until the clinical staff members sign off, so the order is delayed until the chart is signed and a copy of the notes sent to the DME.
Kathleen Schaum has posted an incredibly informative and detailed article in TWC about Medicare audits.
Check out her article and my editorial in TWC to learn more.

Dr. Fife is a world renowned wound care physician dedicated to improving patient outcomes through quality driven care. Please visit my blog at CarolineFifeMD.com and my Youtube channel at https://www.youtube.com/c/carolinefifemd/videos
The opinions, comments, and content expressed or implied in my statements are solely my own and do not necessarily reflect the position or views of Intellicure or any of the boards on which I serve.
