


Of 17 patients with wounds I saw in a single day last week, 11 had lymphedema (64%). They include:
- 1 with a history of prostate cancer radiation
- 1 with congestive heart failure and a history of lung cancer
- 1 with breast cancer lymphedema
- 1 with scleroderma
- 3 with post-phlebitic syndrome
- 4 with long standing venous insufficiency








That’s in one day, and it’s not an atypical day. Lymphedema may not have been the reason they were referred, but it’s often a huge factor in whether wounds get healed or stay healed. Lymphedema may be the most common chronic problem linked to non-healing wounds and in many cases, we don’t actually know why patients have it.
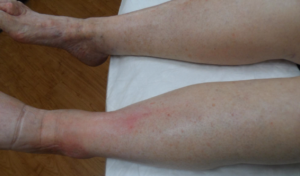
This week I was able to image another patient enrolled in a clinical trial using the Near Infrared imaging technology developed by Eva Sevick. I am not sure how many patients I have imaged with her team in the past 12 or 13 years, but watching the lymphatics function (or not function) in real time never gets old. One of the patients depicted here with profound lymphedema told me hers began when she injured her leg on a concrete step after a golf game. We haven’t imaged her lymphatics, but our experience with similar patients suggests they may have poorly functioning lymphatics (asymptomatic primary lymphedema) that decompensate after minor trauma. We also now know that many common medications can induce lymphedema. Lymphedema probably causes the most frustration for both clinicians and patients.
I think lymphatic disease is the final frontier we need to conquer, but you can’t fight an enemy you can’t see.
NIRF technology is FDA cleared for lymphatic imaging and needs to be widely available. Let’s hope someone will make that happen.
Additional Reading:
Arcanum Aqua – the Mysterious Water Problem of the Lower Extremities

Dr. Fife is a world renowned wound care physician dedicated to improving patient outcomes through quality driven care. Please visit my blog at CarolineFifeMD.com and my Youtube channel at https://www.youtube.com/c/carolinefifemd/videos
The opinions, comments, and content expressed or implied in my statements are solely my own and do not necessarily reflect the position or views of Intellicure or any of the boards on which I serve.
