

Check out the entire series here.
This morning I got an email from a friend and colleague who is one of the best and most ethical wound care practitioners that I know. His letter below points out the problem that started this mess, which is the methodology behind package pricing in the hospital-based outpatient wound center (HOPD).
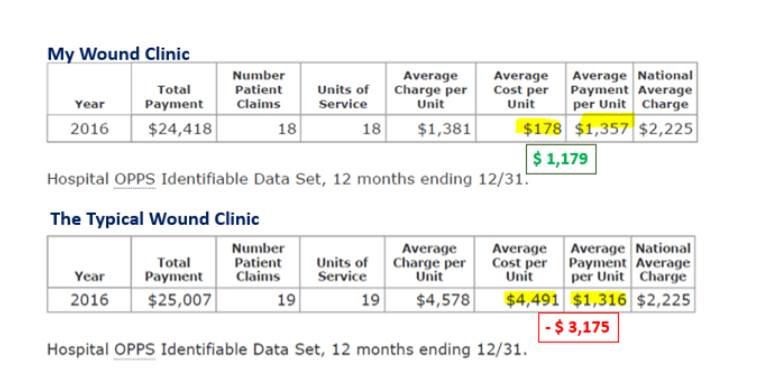
The package price rates were set using flawed CMS data (thanks to hospital computer systems which incorrectly reported “1” piece of product used rather than how many square centimeters). The package price amount when compared to the actual cost of product means that HOPDs can only purchase small products because otherwise they lose money. You can validate this from national data sources. The numbers I quoted in my in 2021 blog were from 2016 because that’s the data to which I had access. However, the situation has not changed.
Most wound centers look like the “Typical Wound Clinic.” In other words, most hospital wound centers are LOSING THOUSANDS OF DOLLARS per application of a cellular product and treating a large ulcer simply can’t be done. The reason that my hospital did not lose money in 2016 is that if a CTP/skin sub cost more than about $1,000, I would not use it. That product cost threshold has crept up a bit since 2016 but refusing to purchase most products (due to cost) is the only way not to lose money in the HOPD. Perhaps that is why the advertisements touting large profits in the doctor’s office frustrate me so much.
HOPDS TYPICALLY LOSE MONEY ON CTP/SKIN SUB APPLICATIONS AND CANNOT TREAT LARGE WOUNDS AT ALL, WHILE DOCTOR’S OFFICES MAKE HUGE PROFITS FROM THE PRODUCT. WHY IS THIS OK?

Dr. Fife is a world renowned wound care physician dedicated to improving patient outcomes through quality driven care. Please visit my blog at CarolineFifeMD.com and my Youtube channel at https://www.youtube.com/c/carolinefifemd/videos
The opinions, comments, and content expressed or implied in my statements are solely my own and do not necessarily reflect the position or views of Intellicure or any of the boards on which I serve.
